Summarized and edited by :
Dr. Amjad Alotaibi , Dr. Hani Alhebshi
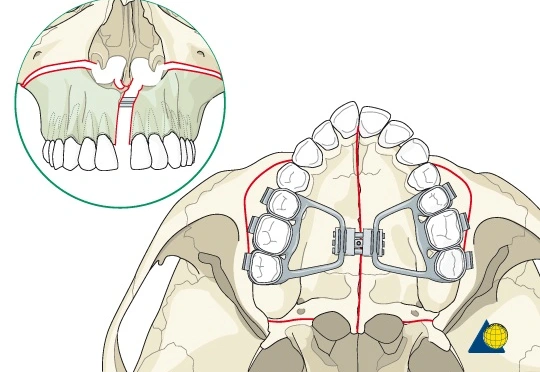
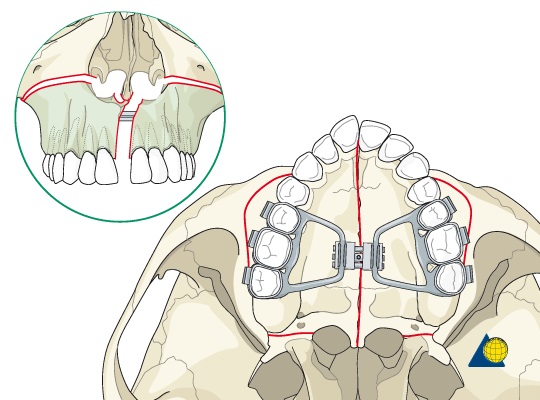
Expansion of the maxillary arch to improve transverse interarch relationships during the primary or mixed dentition stage is considered early transverse treatment as part of a two-phase treatment protocol.
Three possible reasons for early transverse treatment:
- Correct posterior crossbite (The most common)
- Improve arch length deficiency
- Facilitate correction of skeletal class II malocclusions

Posterior crossbite:
Types
Based on the position of the maxillary teeth:
- Posterior lingual crossbite (most common)
- Posterior buccal crossbite
(N.B; Canine involvement is often seen and considered part of a posterior crossbite even though canines are not, by definition, posterior teeth)
Based on the involved side of the arch :
- Unilateral
- Bilateral
Incidence
In the primary and mixed dentition: Estimates range from 7% to 23% with a greater prevalence of unilateral crossbite coupled with a lateral shift of the mandible.
Etiologies
A range of possible causes includes genetics, environmental factors, and habits that result in transverse maxillary skeletal deficiency, asymmetric growth of the maxilla or mandible, discrepant widths of basilar maxilla and mandible, and so on.