Prepared by : Dr. Hani Alhebshi. , Dr, Saleh Alkhathami and Dr.Shehab Kaaki.
This is a thorough overview on the management of Calss II malocclusion.
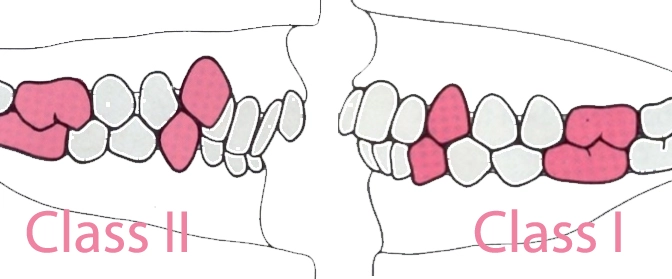
Signs of Class II malocclusion :
- Convex Profile
- Increased overjet
- Skeletal pattern can be due to retrognathic mandible or prognathic maxilla or combination or both.That can be figured out by checking SNA and SNB angles.
- Lips are commonly incompetent.
- Nasiolabial angle is acute espaecially in Class II division I.
- Class II molars , Canines and Incisors.
British school classify malocclusions according to the incisors relation mainly , while american school mainly depends on the molar and canine relation.
Therefore the British consider an increased overjet due to thumb sucking as Class II even if molars and canines are in Class I relation.
In Class II division 1 :
Treatment of class II division I is done sometimes to prevent trauma to maxillary anterior teeth because they are too proclined.
In Class II division 2 :
Upper central incisors are retroclined while laterals are in average or proclined inclination.
Overbite is commonly increased. The retroclined incisors might mask an increased overjet.Canine classification might then be a good parameter to check to confirm the Class II occlusion.
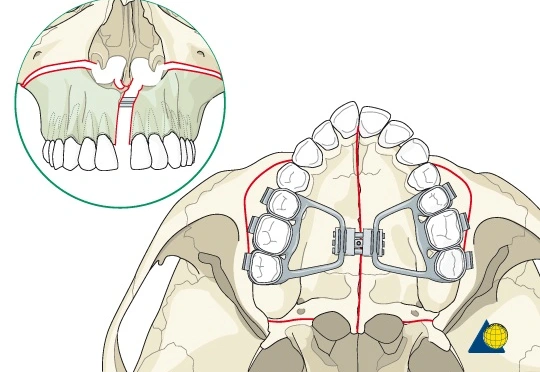
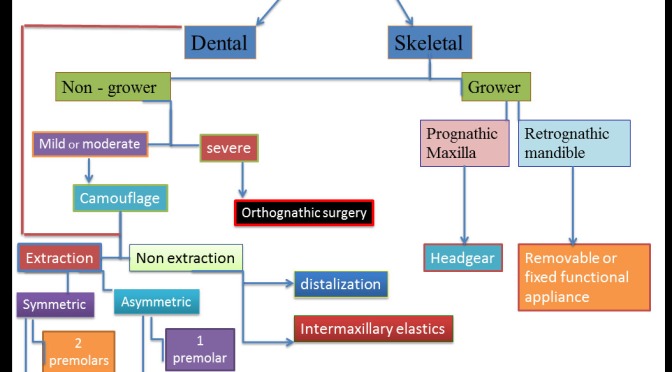
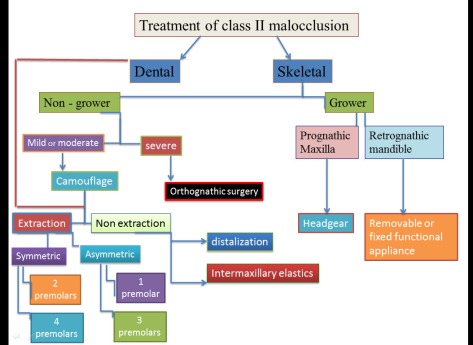
First step in managment : Determine the cause of Class II malocclusion. Is it skeletal or dental ?
If it is a skeletal then it can be due to a prognathic maxilla or a deficient mandible or combination of both.
On Cephalometric radiograph , ANB is oftenly increased ( above 4° ).
Skeletal Age : is the first important parameter that determines the path of treatment.In growing patients , growth modification can be used by the use of functional appliances or headgear while non-growing (adults) patients a camouflage or orthognathic surgery are chosen.
Growth Modification :
When patient is in preadolescence then a growth modification strategy can be considered.
CVM ( Cervical Vertebral Maturation) or hand wrist evaluation will show whether growth is still active or not.
Menarche ( The 1st menstruation cycle in girls ) indicates that growth has passed the peak in females. Ideal time to start growth modification is when CVM at stage 3 meaning that the peak in mandibular growth has occured within one year before this stage.
Therefore , correction of class II can be carried out in this time by inducing mandibular advancement by functional appliances like herbst or twin block appliance. especially when the problem is mainly due to the mandibular retrognathism; or by restraining maxilla by means of headgear to allow mandible to grow and catch up maxillary growth especially when the problem is maxillary prognathism.
The choice between a high pull or cervical headgear depends on the vertical growth pattern of the patient.
If the lower facial height is high (with or without an open bite ) and mandibular plane angle is increased (hyperdivergent) then a high pull or combined headgear should be chosen to prevent extrusion of molars or any increase in the vertical dimension.
On the contrary, low facial height and (hypodivergent mandibular plane) necessate the use of cervical headgear type to allow some extrusion of molars and subsequent overbite correction owed to backward rotation of the mandible.
Orthognathic Surgery:
- In late adolescence or adults (i.e non-growing): Usually a bilateral sagittal split osteotomy is performed to advance the mandible.
- Maxillary setback with impaction can be beneficial too especially if the malocclusion is accompanied by a gummy smile.
- Double jaw surgery can be done in both jaws if the problem is related to a combination of prognathic maxilla and retrognathic mandible.
The decision is better made by the surgeon and the orthodontist after making a visual treatment objective plan (VTO). This will predict the required movements needed to correct the skeletal discrepancy.
Camuoflage :
Camouflage options are useful if patient has mild to moderate skeletal discrepancy or refuses surgical option.That will depend on the severity of Class II.
The soft tissue profile is a critical factor in the treatment plan.Nose and lips position are also other important parameters.
- Camouflage treatment is most often done by extraction of upper 4s with maximum or absolute anchorage finishing molars in Class II while correcting canines into Class I relation.
- Other options include extraction of upper 4s and lower 5s if crowding is severe in lower arch.
- In severely flat profile or very prominent nose , extraction of upper premolars will ruin the profile and dish the face so that it appears uglier than before the treatment. Therefore , surgical approach should be presented to the patient as best option.
- Using Class II correctors like Forsus is a good option unless patient has a severely proclined lower anterior teeth where it is contraindicated.
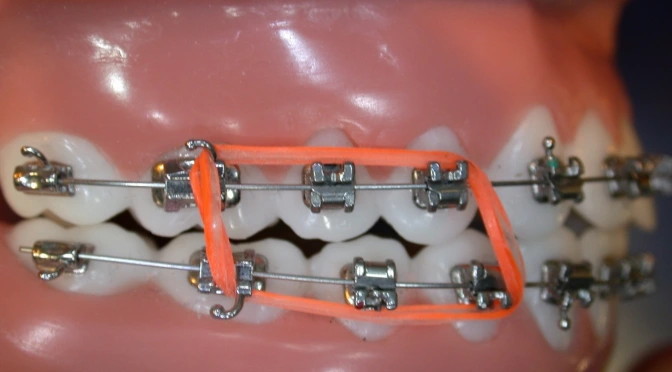
- Class II elastics are also used to correct Class II molars and canines to class I relationship.It should be used cautiously especially when lower anteriors are proclined or vertical dimension is already high before treatment. Thats owing to the effect of class II elastics namely the protrusion of lower incisors , extrusion of lower molars that would increase the vertical dimension.Class II elastics is also contraindicated in gummy smile cases because of their effect in rotating the occlusal plane in a clockwise direction ending up with an increased gingival display.
- Genioplasty ( to advance the chin ) is needed sometimes to correct the retrusive chin usually accompanied with extraction of upper 4s. this option is offered to the patient after the treatment of orthodontics is completed.
Effect of types of treatment on the soft tissue :
- Lips should go back and become competent.
- Nasiolabial angle should increase. ( i.e change from acute to obtuse angle. )